ICSI in 2026: the fertility procedure used in millions of IVF cycles
Intracytoplasmic sperm injection, or ICSI, is one of the most widely used assisted reproductive technologies in modern fertility care. In the United States, the Centers for Disease Control and Prevention reported that assisted reproductive technology contributed to about 2.3% of all infants born in 2022, the latest national ART birth-share figure available in CDC surveillance reporting. By 2026, ICSI remains a routine laboratory method in IVF clinics, particularly for severe male-factor infertility, previous fertilization failure and cases involving limited numbers of eggs or sperm.
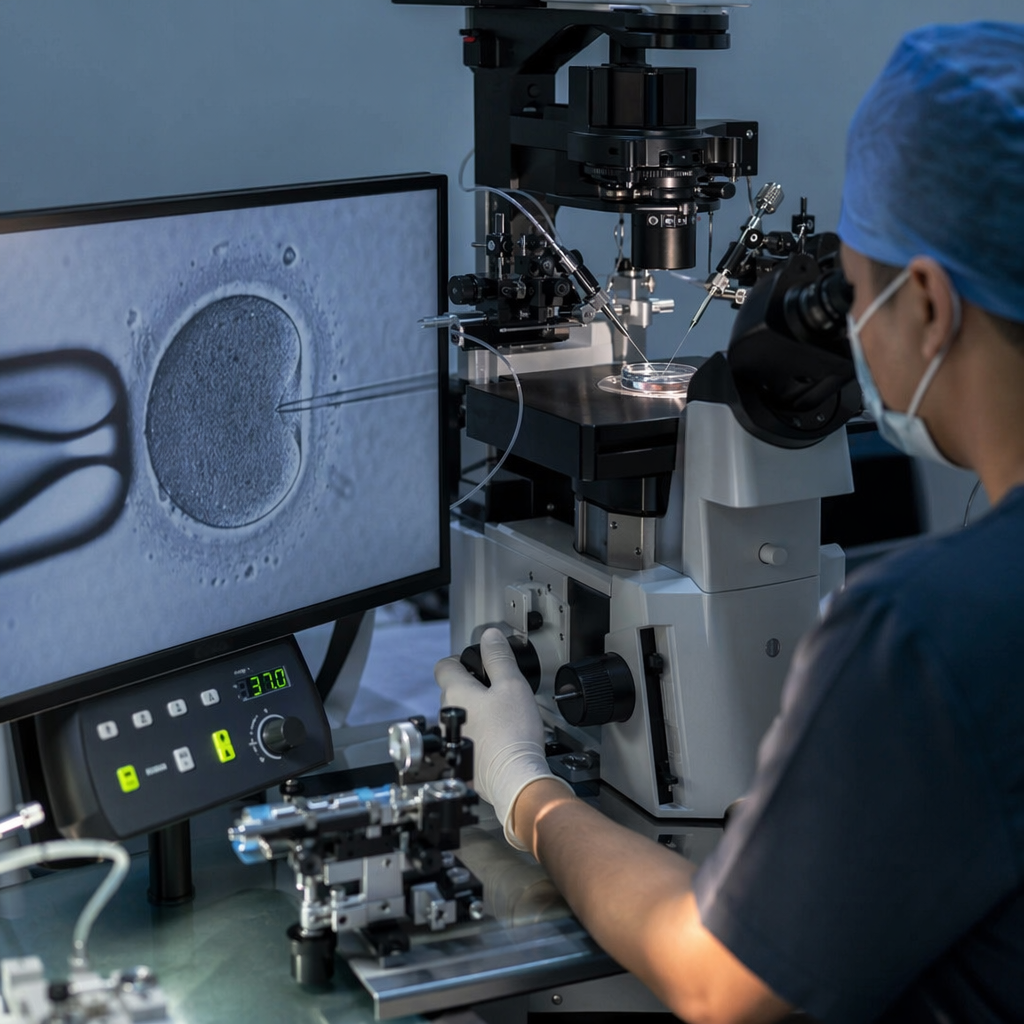
ICSI is not a separate pregnancy treatment from in vitro fertilization. It is a fertilization technique used inside an IVF cycle. Instead of placing eggs and sperm together in a dish and allowing fertilization to occur, an embryologist injects a single sperm directly into the cytoplasm of a mature egg using a fine glass needle under a microscope. The resulting embryo, if it develops normally, can then be transferred to the uterus or frozen for later use.
The procedure has become central to fertility treatment because it addresses a specific biological barrier: sperm that cannot reliably fertilize an egg on their own. However, health authorities and professional societies describe ICSI as a technique with defined clinical indications, not a universal requirement for every IVF patient.
What ICSI is used for
ICSI was developed to overcome fertilization problems, especially those related to sperm count, sperm movement or sperm shape. The UK National Health Service describes ICSI as a technique in which a single sperm is injected directly into an egg, usually as part of IVF treatment. The Human Fertilisation and Embryology Authority, the UK fertility regulator, states that ICSI may be recommended when there is a very low sperm count, poor sperm motility, abnormal sperm morphology, previous IVF fertilization failure, or sperm retrieved surgically from the testes or epididymis.
As of 2026, ICSI is also used in some cycles involving frozen eggs, preimplantation genetic testing, or very low numbers of available eggs, because clinics may seek to reduce the risk of total fertilization failure. The American Society for Reproductive Medicine has said in committee guidance that ICSI is clearly indicated for male-factor infertility, while routine use in non-male-factor infertility has not consistently shown improved live-birth outcomes.
For patients, the ICSI process begins in the same way as IVF. Ovarian stimulation medications are used to encourage the ovaries to mature multiple eggs. The eggs are collected through a transvaginal procedure under ultrasound guidance. A semen sample is prepared in the laboratory, or sperm may be obtained surgically if there is no sperm in the ejaculate. Mature eggs are then injected individually with selected sperm.
Key 2024–2026 data points
Official international ICSI-specific numbers are not published in real time across all countries, because fertility registries often release data after validation. Still, several public datasets and official reports available by 2024–2026 show the scale of assisted reproduction and the regulatory environment in which ICSI is used.
- United States: The CDC reported that ART accounted for about 2.3% of all U.S. infants born in 2022, based on national ART surveillance published in recent CDC reporting.
- United States clinic network: The CDC’s National ART Surveillance System covers more than 450 fertility clinics reporting ART outcomes in the United States in recent annual reports.
- United Kingdom: The Human Fertilisation and Embryology Authority reported that around 52,500 patients had IVF treatment in 2022, in its May 2024 report on fertility treatment trends.
- United Kingdom embryo transfers: HFEA data published in 2024 showed IVF and donor insemination treatment continued after the COVID-19 disruption, with treatment numbers returning close to pre-pandemic levels by 2022.
- India regulation: India’s Assisted Reproductive Technology (Regulation) Act, 2021, and Surrogacy (Regulation) Act, 2021, remained the main national regulatory framework for ART clinics as of 2026, with registration requirements for clinics and banks.
- WHO infertility estimate: The World Health Organization reported in 2023 that about 1 in 6 adults worldwide experience infertility during their lifetime; this estimate remained a key global reference through 2024–2026.
How the laboratory procedure works
ICSI requires specialist equipment and trained embryology staff. After egg retrieval, the laboratory identifies mature eggs, because only mature eggs can normally be injected. The embryologist immobilizes an individual sperm and loads it into a microscopic injection pipette. The egg is stabilized with a holding pipette, and the sperm is inserted directly through the zona pellucida and egg membrane into the cytoplasm.
Fertilization is usually checked the following day. A normally fertilized egg shows two pronuclei, one from the egg and one from the sperm. Embryos are then cultured for several days, commonly to the cleavage stage on day 2 or day 3, or to the blastocyst stage on day 5 or day 6. One embryo may be transferred, depending on age, embryo quality, national rules and clinic policy. Additional suitable embryos can be cryopreserved.
The major distinction between ICSI and conventional IVF is the method of fertilization. Ovarian stimulation, egg retrieval, embryo culture, embryo transfer and pregnancy testing are otherwise broadly similar.
Success rates: what the numbers mean
Success after ICSI depends on many of the same factors that influence IVF outcomes: age of the person providing the eggs, ovarian reserve, embryo quality, uterine factors, sperm factors, previous pregnancy history and clinic practice. National regulators generally report success by IVF cycle type, patient age and embryo transfer, rather than presenting ICSI as a stand-alone guarantee.
The CDC explains that ART success rates vary substantially by age. U.S. ART data consistently show higher live-birth rates among younger patients using their own eggs and lower rates with increasing age. The HFEA similarly reports that patient age is one of the strongest predictors of IVF success. These findings apply to ICSI cycles because ICSI is a fertilization method within IVF.
HFEA public information states that ICSI does not necessarily increase the chance of having a baby for every patient when compared with conventional IVF. Its main purpose is to improve the chance that fertilization will occur when sperm-related or previous fertilization problems are present. The American Society for Reproductive Medicine has also reported that routine ICSI in cases without male-factor infertility has not been shown to improve live-birth rates consistently.
As of 2026, the most evidence-based way to interpret ICSI success is therefore not to ask whether ICSI is “better” than IVF, but whether it is medically indicated in a particular IVF cycle.
Who may be advised to consider ICSI
Clinics may discuss ICSI when semen analysis shows severe abnormalities, including very low sperm concentration, very low motility or a high proportion of abnormal forms. It may also be used when sperm are surgically retrieved, such as in obstructive azoospermia, where sperm production occurs but sperm cannot pass into the ejaculate.
ICSI may also be discussed after a previous IVF cycle in which few or no eggs fertilized with conventional insemination. In such cases, direct injection can reduce the risk of repeat fertilization failure. Some clinics use ICSI for frozen-thawed eggs because the freezing and warming process may affect the egg’s outer layer, making conventional sperm penetration less predictable.
However, professional guidance cautions against assuming that ICSI is needed in all IVF cycles. The decision is usually based on semen results, egg number, reproductive history, laboratory policy and patient-specific medical factors.
Cost and access
ICSI usually adds a laboratory charge to an IVF cycle. Costs vary widely by country, clinic and whether medicines, testing, freezing and embryo transfer are included. In the United States, fertility care is often partly or fully paid out of pocket unless employer or state insurance mandates apply. In the United Kingdom, NHS-funded IVF access depends on local eligibility rules, while private IVF and ICSI costs are listed separately by many clinics. In India, ART clinics are regulated under national law, but pricing varies by provider and city.
Government and regulator data show that ART access remains uneven. The WHO has reported that infertility affects people globally, but access to diagnosis and treatment is limited by cost, availability and legal frameworks. In countries without comprehensive fertility coverage, ICSI may be clinically available but financially inaccessible for many patients.
As of 2026, many clinics also charge separately for related services such as sperm retrieval, preimplantation genetic testing, embryo freezing, storage and frozen embryo transfer. Patients are advised by regulators such as the HFEA to request a full written cost breakdown before starting treatment.
Risks and safety issues
ICSI is performed on eggs outside the body, but the wider IVF process includes medical and procedural risks. Ovarian stimulation can cause side effects, including bloating and discomfort. A rare but serious complication is ovarian hyperstimulation syndrome. Egg retrieval carries small risks of bleeding, infection and injury to surrounding structures.
For pregnancies resulting from IVF or ICSI, the risk of multiple pregnancy depends mainly on how many embryos are transferred. Regulators in several countries have encouraged elective single embryo transfer for many patients to reduce twin and higher-order multiple pregnancies, which are associated with higher risks of preterm birth and low birth weight.
Some studies have examined whether ICSI is associated with congenital anomalies or developmental outcomes. Public health agencies generally emphasize that separating the effects of ICSI from underlying infertility factors is difficult. The CDC and other authorities continue to monitor ART outcomes through national surveillance. Professional counselling typically includes discussion of known uncertainties, especially when ICSI is used for severe male-factor infertility that may have a genetic component.
When sperm counts are extremely low or azoospermia is present, clinicians may recommend genetic evaluation, such as karyotype testing or Y-chromosome microdeletion testing, depending on the clinical findings. This is because some causes of male infertility can be inherited and may be passed to male offspring.
ICSI and male infertility
Male-factor infertility is a major reason for ICSI use. Semen analysis assesses sperm concentration, motility and morphology, but results can vary between samples. Causes of male infertility include varicocele, hormonal disorders, infections, genetic conditions, obstruction, prior surgery, cancer treatment and some medications.
ICSI can help when sperm are present but unable to fertilize an egg effectively. It does not treat the underlying cause of male infertility. For that reason, reproductive urologists may evaluate men before ICSI, particularly when sperm counts are very low or sperm must be surgically retrieved.
Surgical sperm retrieval methods include percutaneous epididymal sperm aspiration, microsurgical epididymal sperm aspiration, testicular sperm aspiration and microdissection testicular sperm extraction. The choice depends on whether azoospermia is obstructive or non-obstructive. Retrieved sperm can often be used fresh or frozen for later ICSI cycles.
Regulation and reporting
ART regulation differs widely between countries. In the United States, the Fertility Clinic Success Rate and Certification Act requires clinics to report ART success-rate data to the CDC. The CDC publishes annual clinic-level and national ART reports. In the United Kingdom, the HFEA licenses and monitors fertility clinics and embryo research, publishes inspection reports and provides patient-facing treatment data.
India has introduced national ART regulation through the Assisted Reproductive Technology (Regulation) Act, 2021. The law sets registration requirements for ART clinics and banks, outlines duties of clinics, and creates national and state boards. As of 2026, ART providers in India are expected to operate within this statutory framework.
These systems matter because ICSI outcomes depend not only on clinical indication but also on laboratory standards, embryo handling, record keeping and transparent reporting. Public reporting allows patients to compare broad clinic performance, although regulators caution that success rates must be interpreted in context because patient populations differ.
What patients are commonly told before treatment
Before ICSI, clinics typically explain the reason for recommending the technique, the expected fertilization plan, what will happen if few eggs are collected, and whether sperm retrieval or donor sperm is being considered. Consent forms generally cover egg collection, sperm preparation, injection, embryo culture, embryo transfer, freezing and storage.
Patients may also be counselled that not every mature egg will fertilize after ICSI, and not every fertilized egg will develop into a transferable embryo. Pregnancy is not guaranteed after embryo transfer. National ART data from the CDC and HFEA show that outcomes vary strongly by age and clinical circumstances.
As of 2026, ICSI is best understood as a targeted laboratory solution for fertilization problems within IVF. Its most established role remains severe male-factor infertility and previous fertilization failure. For patients without those indications, the available guidance from regulators and professional societies supports individualized counselling rather than routine use for all IVF cycles.
Sources: Reuters, Government releases, publicly available data.
Comments
Post a Comment